CALCIFIC TENDONITIS OF THE SHOULDER
- Alain Iserin

- Jul 16, 2024
- 4 min read
Updated: Jul 19, 2024
INTRODUCTION
Calcific tendonitis of the shoulder is a fairly common cause of shoulder pain before the age of 40. This pathology involves especially women between 25 and 40, and commonly both shoulders. Very sudden and acute pain may occur. Calcific tendonitis has no relation with tendon wear, quality of food or an eventual notion of trauma.

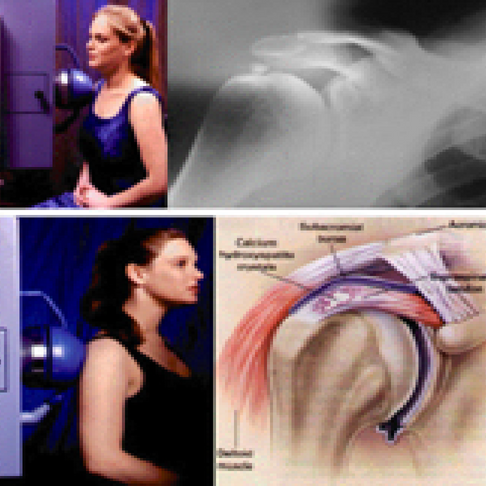
ANATOMY ET PHYSIOLOGY
The rotator cuff is formed by three main muscles which attach by their tendons to the superior aspect of the humerus, surrounding the humeral head at the level of the shoulder joint.
This group of muscles and tendons creates the strength to lift and rotate the arm. It also contributes to the stability of the shoulder.
Those tendons named supra-spinatus, infra-spinatus or sub scapularis may carry, close to their humerus attachment, a calcific deposit in the depth of the tendon itself. This calcific deposit is probably related to a lack of oxygen at the insertion site of the tendon. This pathology has no relation with tendon wear, trauma or type of food.
At first the size and the volume of the calcific deposit increases progressively, and then for an unknown reason suddenly may begin to disappear associated to an acute pain syndrome. Sudden calcium release in the shoulder joint creates a massive inflammatory reaction leading sometimes to an acute pain crisis day and night. This phenomenon is unexplained and the moment of this sudden release is unpredictable.
SYMPTOMS
The presence of a calcific deposit at the origin of a shoulder tendon may be completely free of pain and symptoms. But most of the time pain occurs and move to 2 possible ways:
- a « chronic » way with daily pain, that increases with movement but also present at night,
- an « acute » way, leading to an unbearable and extreme pain crisis.
DIAGNOSIS
When pain takes a chronic evolution, symptoms look very much alike the impingement syndrom. Physical examination shows evidence of catching between the calcific deposit and the bone above, the acromion (the superior part of the scapula).




In the acute phase, shoulder mobility is diminished and every attempt to move the arm is extremely painful. This situation can lead to a secondary stiffness of the shoulder joint.
A standard radiograph is sufficient to establish the diagnosis. Calcific tendonitis is hardly ever associated with rotator cuff tendons tears
During the chronic phase, the calcific deposit takes a round, well limited, and condensed aspect, situated close to the insertion site of the tendon onto the bone.




In the acute phase, very often, the Xray shows signs of spontaneous disappearance of the calcium such as elongated aspect along the tendon.
Radiologic aspect may vary regarding the phase of the disease. A recent Xray is necessary to assess the precise situation of the calcific deposit disease.
An ultrasound may sometimes be needed to diagnose little or scattered deposits and precise their location
MRI is rarely necessary in this matter
TREATMENT
Conservative treatment
During the chronic phase, anti-inflammatory medications or one guided cortisone injection in the sub-acromial space performed under Xray or ultrasound control may relieve pain at least for a few months
In the acute phase, when the pain is unbearable, a guided cortisone injection will be performed as quickly as possible
Calcific puncture under X Ray or barbotage
This maneuver consists in trying to remove the calcium using a needle guided by Xray.
During the chronic phase the deposit is nearly solid. It maybe illusory to try to remove the whole of the deposit through this puncture. A partial removal may lead to constant pain and difficulty to remove the rest in surgery if necessary.




During the acute phase, the deposit turns nearly into fluidand the puncture seems easier but inappropriate because in this case the calcium disappears most of the time by itself
Indications for tendons puncture or barbotage are therefore very seldom
Shockwave therapy
It is a very powerful anti-inflammatory tool that can relieve pain in its acute phase or when the calcific deposit is too little to be removed arthroscopically.



Arthroscopic removal
Arthroscopic removal through key holes is indicated whenever the symptoms are disturbing for everyday life or for sleep and when the calcific deposit shows a regular and very condensed aspect on standard X rays
Arthroscopic removal (endoscopy) is performed through 2 key holes, under general anesthesia. An incision at the back of the shoulder is used to introduce the endoscope while another one is necessary to introduce instruments.




The calcific deposit is not located at the superficial side of the tendon but rather in the tendon depth This situation justifies a short incision along the tendon fibers that allows a complete removal of the calcium with a curette. This procedure takes about 20 minutes and may be performed as a day case
POST OPERATIVE CARE AND PYSIOTERAPY
Following surgery, the arm remains free to move and the patient does not carry any sling. Pain decreases progressively with time and may take 3 to 6 months to disappear. On X Ray calcific deposit will take weeks to be erased completely after an endoscopic removal.
Once the calcium is gone the patient is definitely cured because the tendon returns to a normal aspect without any degenerative changes.
Physiotherapy is very simple and most of the time will be carried out by the patient himself. Lying on his bed the patient will move the operated arm in forward elevation helped by the other arm using a stick held in both hands (passive motion) Physiotherapy should never be painful. The aim of this exercise is to recover gently a normal mobility.


COMPLICATIONS
Very few complications occur after this procedure but the patient has to remind that pain will be relieved progressively after surgery sometimes in months.
Some kind of post-operative stiffness or « frozen shoulder » remains possible, but mobility will always recover even if it takes time. This phenomenon is related to the sudden release of a massive quantity of calcium leading to an acute inflammatory reaction.
The incidence of post-operative frozen shoulder may be reduced by an immediate cortisone injection in the shoulder.
Infection is a very seldom complication of shoulder arthroscopy.
SUMMARY
Calcific tendonitis of the shoulder is a very common pathology involving young patients, mainly women, giving sometimes very acute pain, which is hardly never associated with wear and tear of the rotator cuff tendons. Treatment depends on the intensity of the pain, and on the Xray aspect of the deposit. If pain becomes unbearable calcium may be easily removed arthroscopically.


Comments